本帖最后由 滴水 于 2012-5-24 21:29 编辑
- S! y& H# V, v$ k% [& c' o( q, r; c' o. q
5月22日:今天上午咳出好多血,看得我害怕,吃了3颗云南白药好点了。9 i+ E9 K5 W- E
验血报告出来了,在电脑上看的,胆红素、血小板 、凝血都是正常的。那咳血是什么原因呢?今天才知道老爸从5月2日起一直在吃云南白药,最近停了6天。
% o* g' \0 ]* I6 B n# c/ |血常规忘了看了,但医生有说过是正常的。# f% {. X/ o6 D4 }0 w# U- Z% r
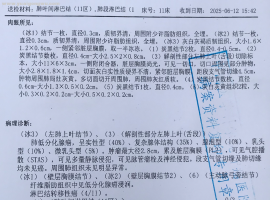
今天做了增强CT,报告要明天出来,今夜注定要辗转反侧了。。。
( w5 S* @& Z/ t5 O8 Y
3 y- p2 V5 N$ f" C9 l* a/ q7 c3 F! i2 p
在CT报告出来前,无法区分是肿瘤进展了还是特罗凯的副作用,不管是哪种情况,都要停药: m6 e& [0 U% z* a8 X& }$ U
% E2 D& s) ?0 ]0 PWhat are the possible side effects of Erlotinib?
8 ~, H4 C: R- W! q# g; W) P1 H
: N% Y2 i' I9 \# n% ^8 ?% UGet emergency medical help if you have any of these signs of an allergic reaction: hives; difficult breathing; swelling of your face, lips, tongue, or throat.4 c" E, o6 x5 W
) U# T( q. e7 ]Stop taking erlotinib and call your doctor at once if you have a serious side effect such as:
& n3 F p9 n9 h; c% u9 X8 Vnew or worsening lung problems such as chest pain, dry cough with fever, wheezing, rapid breathing, feeling short of breath: m/ Q7 E5 t4 Y/ ^( H$ X( `0 M
chest pain spreading to the arm or shoulder, nausea, sweating, general ill feeling) D% }$ L% D$ q5 u5 q w' g* t
sudden numbness or weakness, sudden severe headache, or problems with vision, speech, or balance
2 t3 s8 _8 B3 t4 O! seye pain, redness, or irritation
! `0 d) S6 _' g, @2 sconfusion, mood changes, increased thirst, urinating less than usual or not at all
2 ^; s& m( C$ I* u2 Rswelling, rapid weight gain: V( Z9 j' \3 {; B' \: j
severe or ongoing diarrhea, vomiting, or loss of appetite
" {2 p& }0 }8 kblack, bloody, or tarry stools
/ D8 p% R( {' l& v& P: hcoughing up blood or vomit that looks like coffee grounds5 q4 Z) _9 t1 f1 g Q4 a
pale or yellowed skin, easy bruising, unusual bleeding (nose, mouth, vagina, or rectum), purple or red pinpoint spots under your skin
7 d( l h7 X+ P$ I9 n; bwhite patches or sores inside your mouth or on your lips
! u$ I6 c: t. Z; _1 S: ~2 B* s3 Kfever, sore throat, and headache with a severe blistering, peeling, and red skin rash" c s- j! h( K; a: T
the first sign of any type of skin rash, no matter how mild; or$ ~: ]6 t2 e2 C# z3 [
nausea, upper stomach pain, itching, dark urine, clay-colored stools, jaundice (yellowing of the skin or eyes)# v2 I' _: C8 h3 I' O5 D: ]
* |0 J+ T" X' g% uThis is not a complete list of side effects and others may occur. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
% ?, X; o; k$ }6 B) _) g8 x* d' H- C6 _
每隔一阵子就会出现一个处理很棘手的状况9 `$ `7 z) D, k; a* z% r/ x) r" F" q
|
 老公刚刚54岁,确诊肺癌,手术中发现
各位朋友好。
度过了慌乱的一个月,有机会发现了这个论坛,如获至宝,说说我家
老公刚刚54岁,确诊肺癌,手术中发现
各位朋友好。
度过了慌乱的一个月,有机会发现了这个论坛,如获至宝,说说我家
 父亲肺鳞癌,cT3N0M1a,ⅣA,脑转移
父亲2025年6月中旬因为头痛,一侧肢体不灵活入院,做了增强核磁,发现右侧额叶占位(3
父亲肺鳞癌,cT3N0M1a,ⅣA,脑转移
父亲2025年6月中旬因为头痛,一侧肢体不灵活入院,做了增强核磁,发现右侧额叶占位(3
 SMARCA4-NSCLC 盲试靶向药有效!!
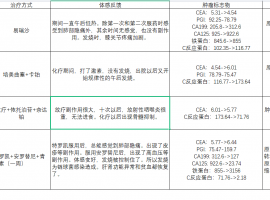
首先感慨一下今天真的是个好日子。努力了进三个月的治疗终于有了重大进展。
复查结果
SMARCA4-NSCLC 盲试靶向药有效!!
首先感慨一下今天真的是个好日子。努力了进三个月的治疗终于有了重大进展。
复查结果
 希望给没有阅读过的人一些体会
本文来自于此书,只是做一些摘抄,分享给深陷迷茫的人。文中观点真实与否,效果怎么
希望给没有阅读过的人一些体会
本文来自于此书,只是做一些摘抄,分享给深陷迷茫的人。文中观点真实与否,效果怎么
 L858R+S768I+TP53阿法替尼用药半年希
2023.11.23我父亲(63岁)因胸腔积液,呼吸困难,后背疼,声音沙哑入院。此前一个多月
L858R+S768I+TP53阿法替尼用药半年希
2023.11.23我父亲(63岁)因胸腔积液,呼吸困难,后背疼,声音沙哑入院。此前一个多月





 显身卡
显身卡

 7 P" w% E* h8 ~( t6 B
7 P" w% E* h8 ~( t6 B


